
It’s not until a few years ago that we developed a 3D animation project, the cranio-facial-universe.com (CFU), destined for teaching and dental research, in collaboration with Lille II faculty. The CFU is also a conceptualization project. In fact, the fundamental data (the genetics and the acquired), and the analyses and clinical findings concerning the essentiality of the mandible led us to the Three-dimensional Mandibular Concept and then to the Morpho-Functional Mandibular Rehabilitation. But since we have to consider the whole cranio-facial entity to accomplish rehabilitation, this new concept of global Rehabilitation was given a new name: Morpho-Functional Cranio-Facial Rehabilitation (RCFMF). This recovery process is physiological, skeleto-muscular, gnathological and functional. The RCFMF consists of « the morpho-functional model »: the FIVE entities that constitute the masticatory apparatus (fig. 2.1), and that, when harmonious, led us to the identification of the FOUR conditions of the act of manducating (fig 2.2): Functional Centric Relation (1st condition), straight Opening and Closing movement (2nd condition), Physiological Occlusion (3rd condition) and Functional Chewing. These conditions constitute the normal functioning of the masticatory apparatus (FAM). According to this and when one or more entity is disordered, the mastication is not normal. This is the definition of the Disorders of the Manducatory Apparatus (DAM) of the RCFMF, also called « the morpho-Dysfuncional model », which gives us a new classification based on the etiopathogenesis of the different minor or major adaptive or pathological syndromes (fig. 2.3). The temporary or permanent treatments (Dentofacial orthopedics, occlusal balancing via a mandibular guide, prosthetics, posturology,…) should aim for the preservation or the reproduction of the five entities and the four conditions. This is the Morpho-Functional Cranio-Facial Rehabilitation. Note : the figures are appointed 2.1, 2.2 … (2. expresses article 2).
THE « MORPHO-FUNCTIONAL MODEL »:
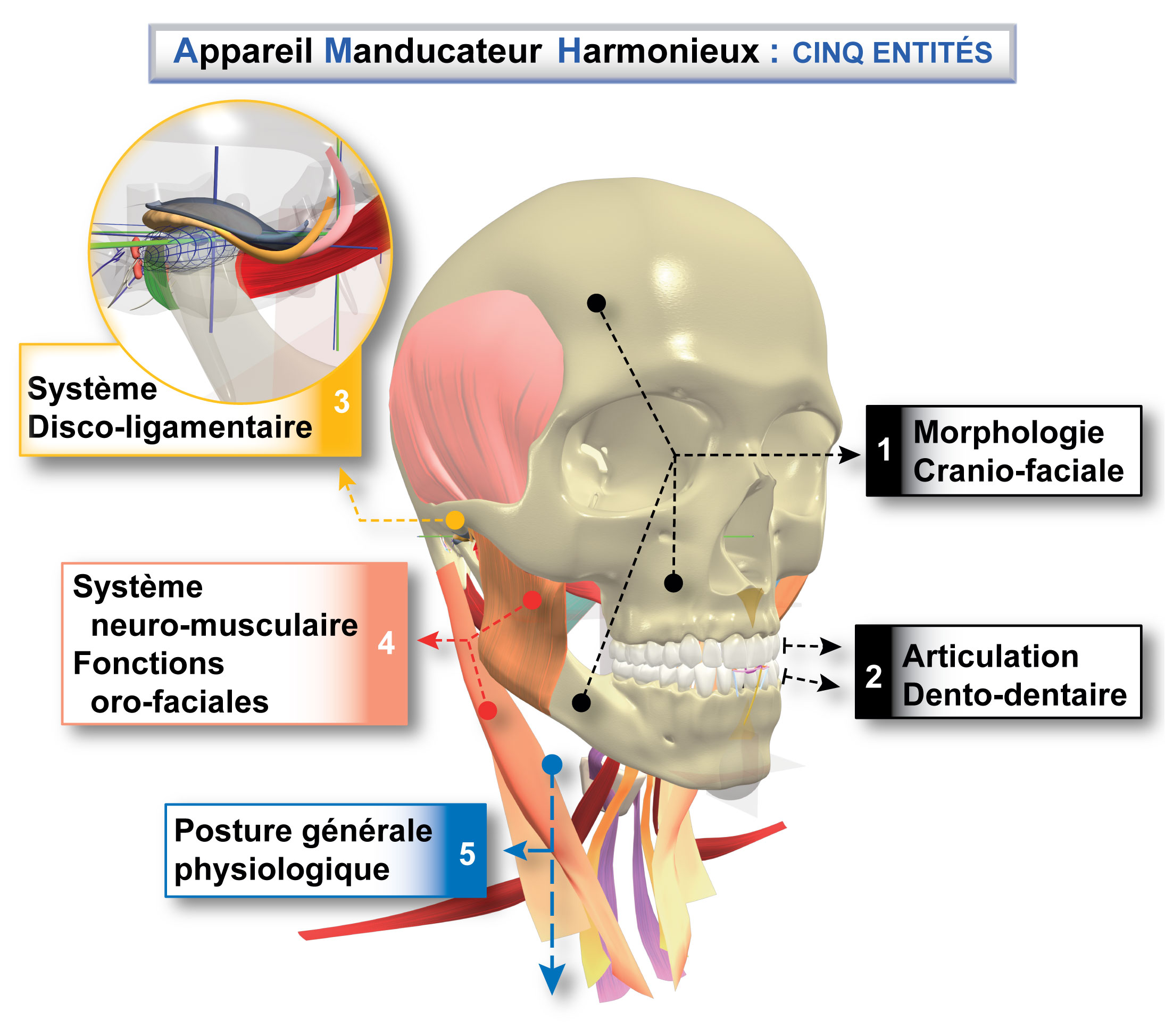
Figure 2.1 the five harmonious entities of the Manducatory Apparatus : 1- Cranio-facial morphology, 2- Dento-dental articulation, 3- Disco-ligamental system, 4- Neuro-muscular system, oro-facial functions, 5- General physiological posture.

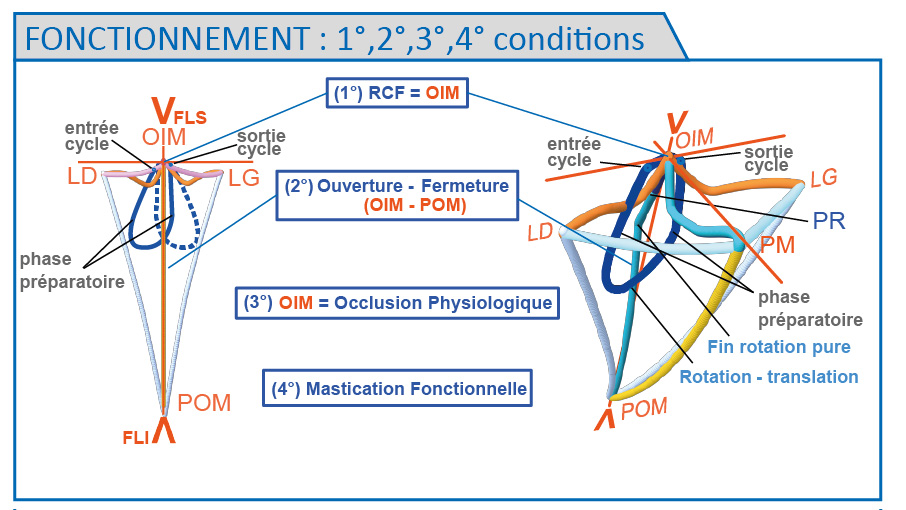
Figure 2.2 New notions: the four conditions of a balanced manducation that represent the (physiological) functioning of the Manducatory Apparatus or FAM
1) RCF, ERCP- reciprocity-2) Prehension: straight Opening and Closing 3) Physiological occlusion 4) Functional mastication. Swallowing: pharyngeal first phase (reflex)-Oro-facial functions.
Functioning of the four conditions: cycle opening, cycle closing.
THE « MORPHO-DYSFUNCTIONAL MODEL »:
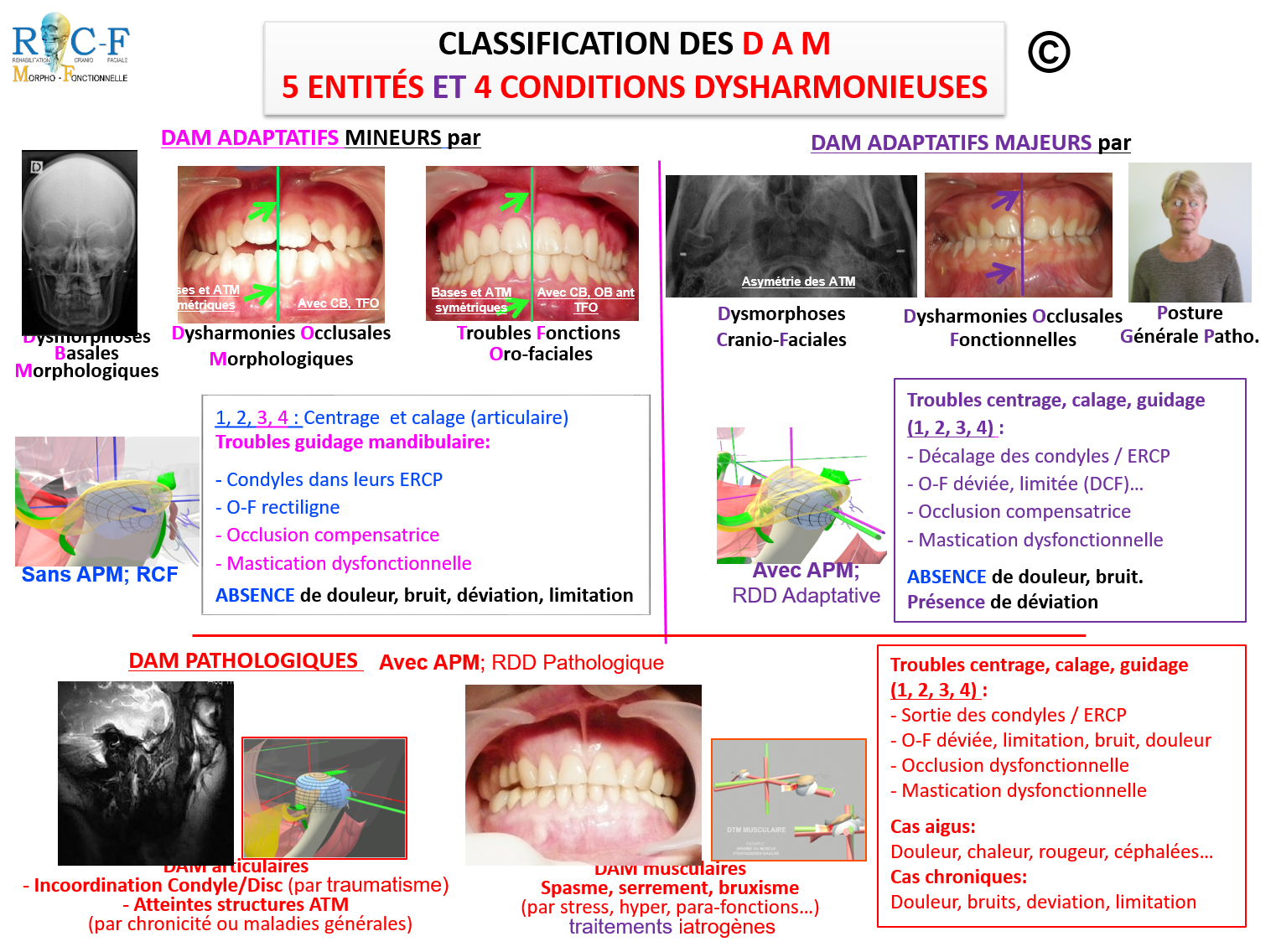
Figure 2.3 DAM classification: etiology, clinical symptoms according to the RCFMF (Unbalanced entities and manducation)
MINOR ADAPTIVE DAMs (1, 2, 3, 4) via:
- Isolated basal dysmorphoses
- Morphological occlusal dysharmonies
- Oro-facial functions disorders
Articular centering and settling, mandibular guidance disorder:
Straight Opening and Closing, compensating occlusion, dysfunctional mastication
Absence of: pain, popping, clicking, deviation, limitation
MAJOR ADAPTIVE DAMs (1, 2, 3, 4) via:
- Cranio-facial dysmorphoses
- Functional occlusal dysharmonies
- Pathological general posture
Centering, settling and guidance disorders:
Condyles shifting, Deviated and limited Opening and Closing, compensating occlusion, dysfunctional mastication
Absence of: pain, popping, clicking
Presence of a shift
Pathological DAMs (1, 2, 3, 4) :
- Articular DAMs, condyle/disc uncoordinated (after a trauma), affected TMJ structures (chronic disease or general syndrome)
- Muscular DAMs: spasms, bruxism, grinding (caused by stress, hyper/para-functions)
Centering, settling and guidance disorders: releasing of the condyles, Deviated and limited Opening and Closing, popping, clicking, pain, dysfunctional occlusion and mastication
Acute cases: pain, heat, redness, headache
Chronic cases: pain, popping/clicking, shifting, limitation
Other etiologies: iatrogenic treatments
In a previous article, we presented the morpho-functional model with the functioning of the manducatory apparatus, or the Normal. The following describe the details of the four conditions of the FAM (Figures 2.4 to 2.7).
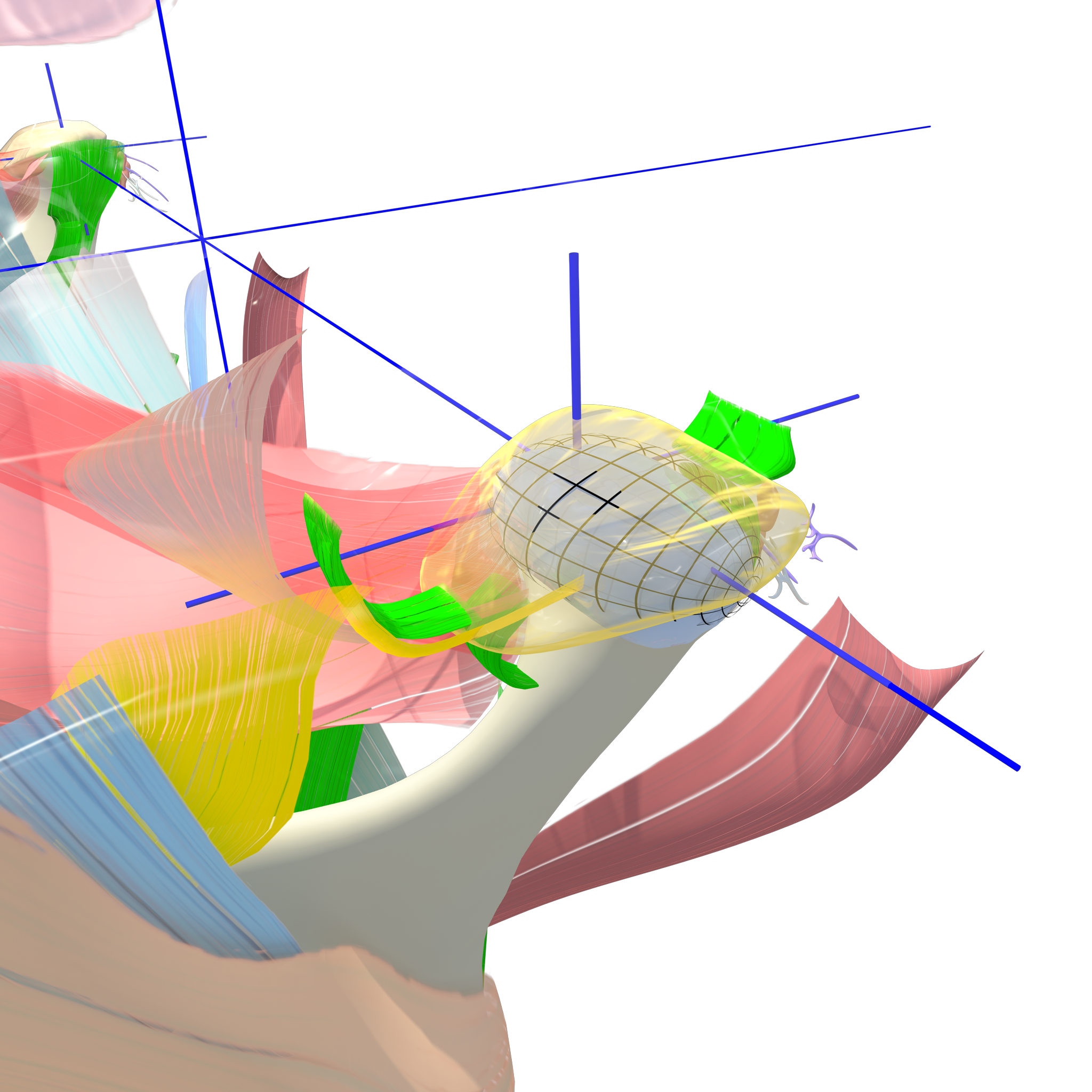
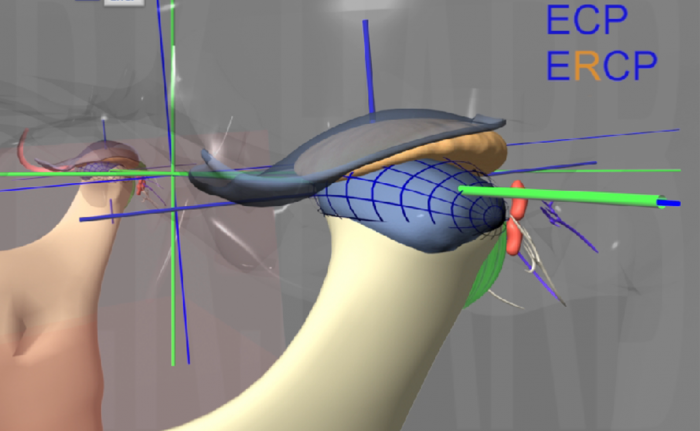
Figure 2.4 First condition: the condyles are in a Functional « Centric » Relation in the physiological condylar rotation space ERCP (grey grid space). This is not an anatomical position, it is a skeleto-muscular position related to the five entities and to the straightest opening-closing movement (second condition) and reciprocally.
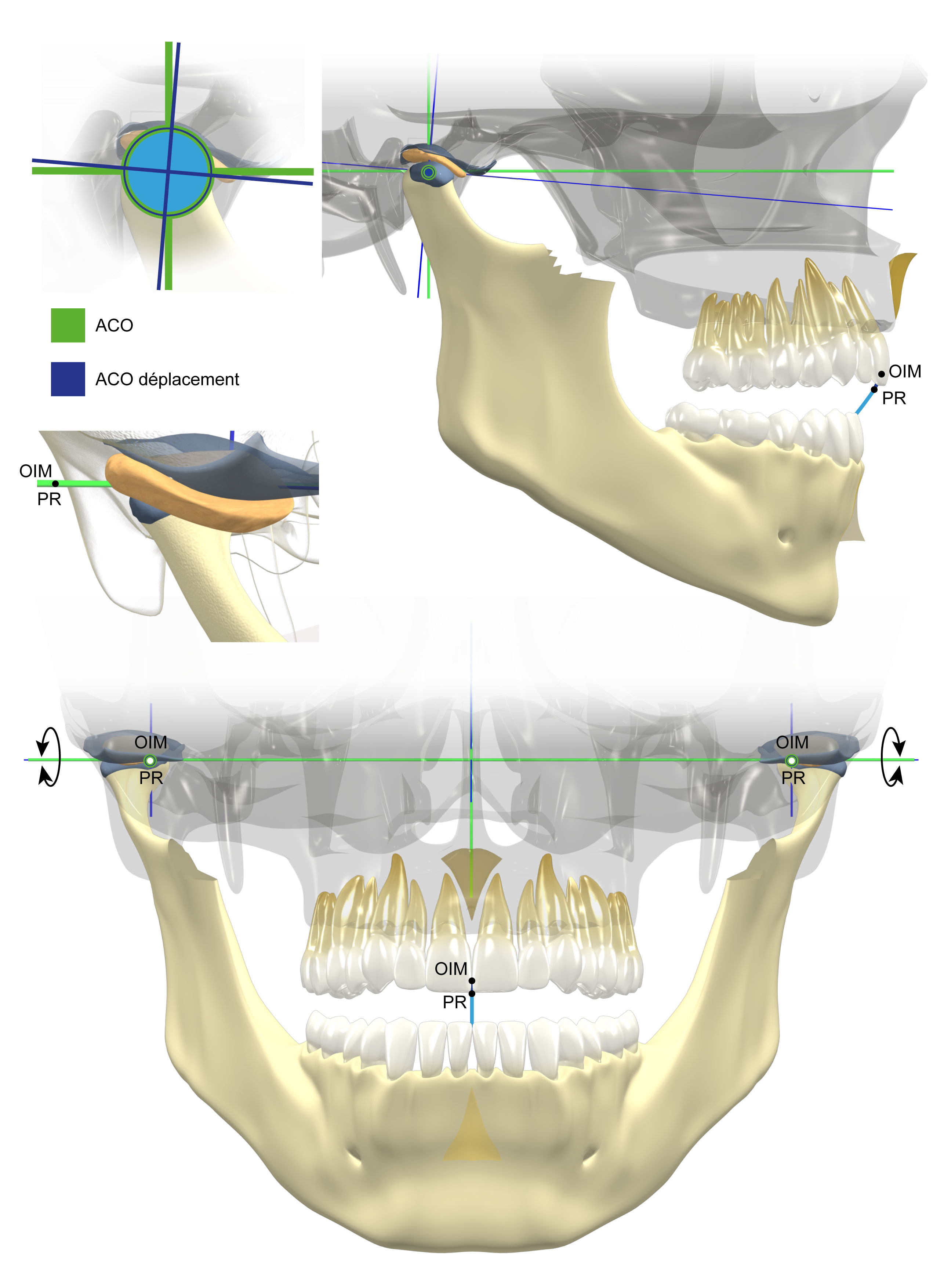
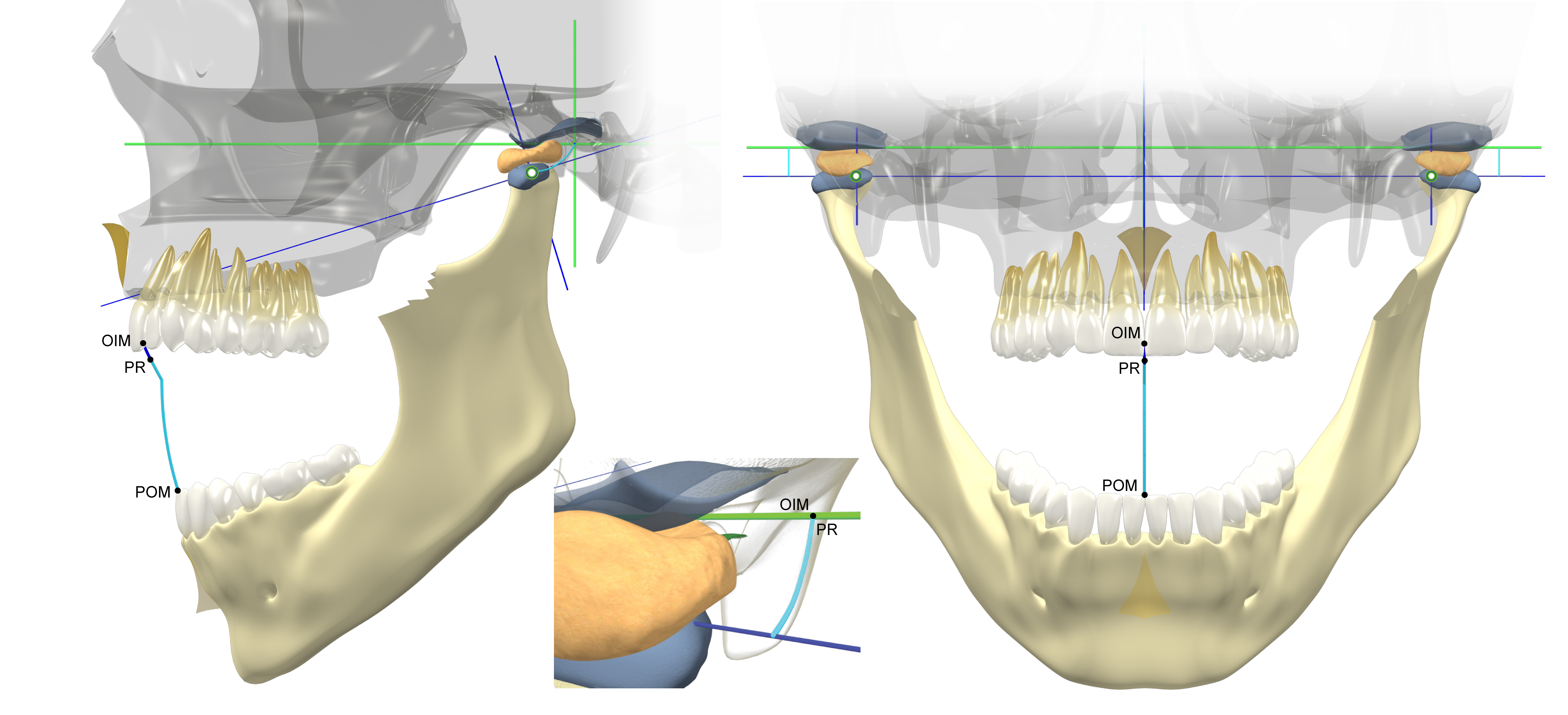
Figure 2.5 Second condition: the straight opening-closing movement is composed of:
- The Mac Collum hinge axes that pass through the medial poles of the condyles (original axes in green, movement axes in blue): the pure condylar rotation in the profile and facial views happens in the 20 mm from the opening start till the closing end.
- The pure rotation is followed by a rotation-translation movement from the OIM, to the relaxed occlusion to the maximal opening position.
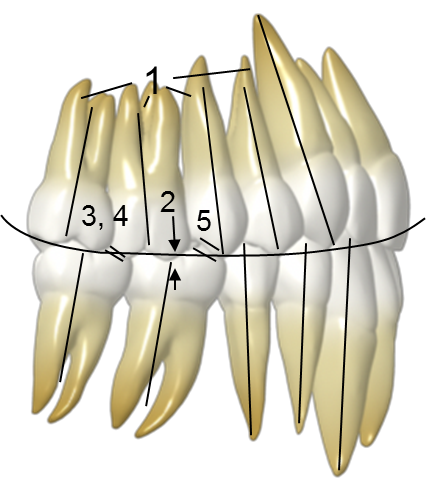
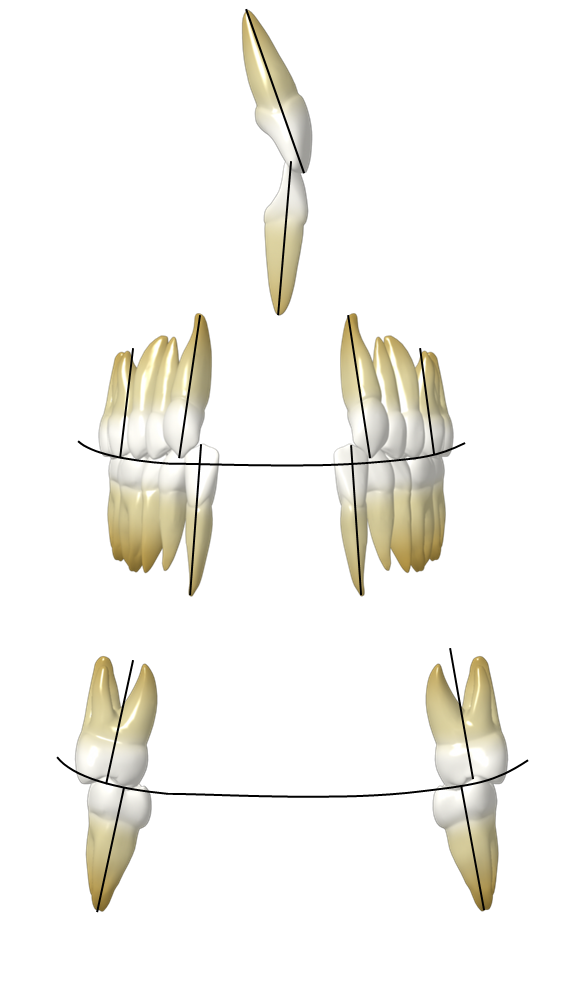
Figure 2.6 third condition: physiological occlusion close to the natural denture:
- The six keys of Andrews, slight curve of Spee
- Positive torque of the lateral sectors (curve of Wilson)… connected directly to the functional mastication (fourth condition) and reciprocally.
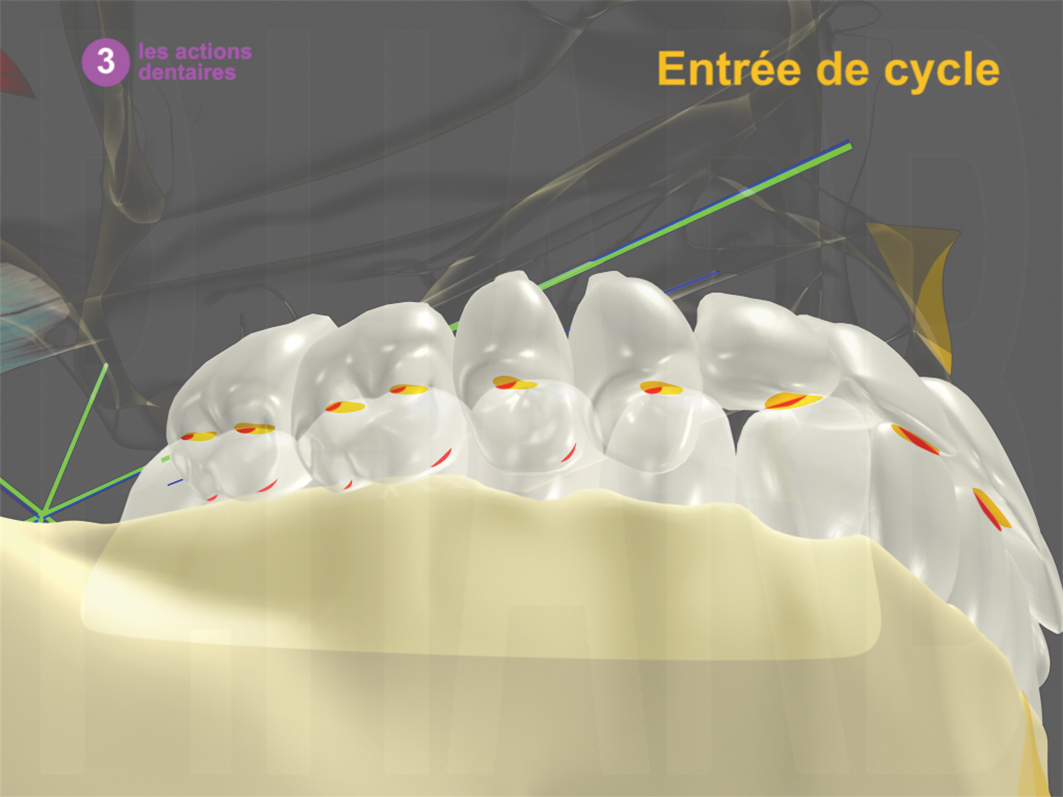
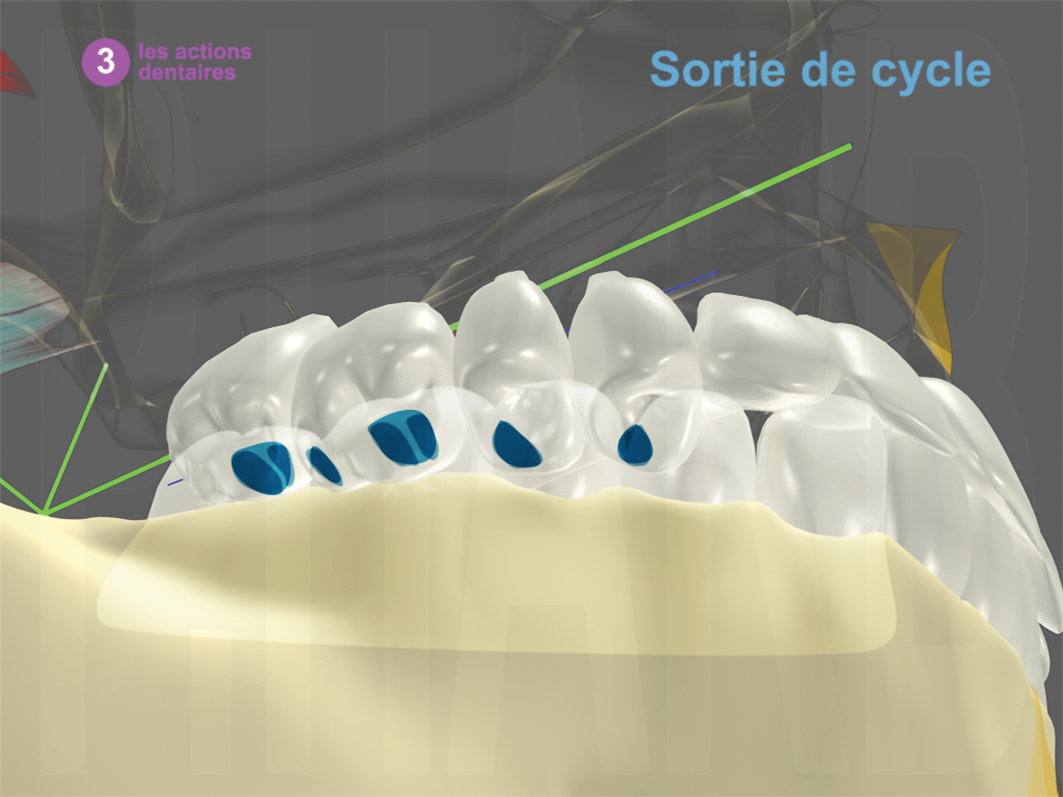
Figure 2.7 fourth condition: functional mastication described by Le Gall and Lauret.
- At the cycle opening, there is the intervention of the jaw elevators, and not the jaw depressors solicited in the canine protected occlusion, and there is the dental contacts from the lateral incisor till the second molar
- At the cycle closing, on the palatal cusp surfaces, related directly to the criteria of the physiological occlusion (figure 2.6)
Our diagnosis and treatment should preserve or reproduce the five entities and the four conditions of the manducation.
In the next article, we are going to discuss the morpho-dysfunctional model with the detailed classification of the DAMs or the Abnormal of the RCFMF.
BIBLIOGRAPHIE
- Aknin J.J. la croissance crânio-faciale édition SID 2007.
- Andrews Laurence F. The six keys to normal occlusion, American journal of orthodontics, 62, p. 296-309 septembre 1972.
- Carels C. Génétique et complexe dento-facial. Orthod Fr. 77. 2006. 79-84.
- Carpentier P., Felizardo R., Yung JP., Clèdes G. L’ATM : le sens du mouvement. Rev Orthop Dento Faciale 2011; 45:127-141.
- Cazzani G. Occlusion et orthodontie Quelques implications pratiques (La Spezia) ODF, XII : 385-396, 1978.
- Cretot M. Aspect morpho-fonctionnel de la courbe d’occlusion. Cahiers de Prothèse 1986;55:153-66.
- D’Amico A. The canine teeth: normal functional relation of the natural teeth of man. J South Calif Dent Assoc 1958; 26: 6-23, 49-60, 127-142, 175-182, 194-208, 239-241.
- D’Amico A. Functional occlusion of the natural teeth of man. J Prosthet Dent 1961; 11-899-915.
- Delaire J. Croissance et morphogenèse du squelette cranio-facial Applications en orthopédie dento-faciale. Orthod Fr Volume 73, Numéro 1, Mars 2002.
- Delaire J. Essai d’interprétation des principaux mécanismes liant la statique à la morphogénèse céphalique. Déductions cliniques AOS, n°130, 1980 ; 189-219.
- Delaire J. Le développement “adaptatif” de la base du crâne. Justification du traitement précoce des dysmorphoses de classe III. Rev Orthop Dento Faciale. 37. 2003. 243-265.
- Delcambre Th. Biomécanique de l’articulation temporo-mandibulaire et dimension verticale. Thèse de Doctorat LILLE
- Gaspard M. L’appareil manducateur et la manducation. 1e partie. Vol. 1 et 2. Paris: J Prélat; 1978-79.
- Gibbs CH., Lundeen HC. Jaw movements and forces during chewing and swallowing and their clinical significance. In: Advances in occlusion. Boston: JohnWright PSG; 1982. p. 38.
- Harb Ph (K), Thilloy G, Delachapelle C, Danguy M. – Biométrie mandibulaire en norma axialis. Proposition d’analyse et de diagramme architectural. Group Intern Rech Sientif Stomato Odontol 3-4:141-150, Palerme 1988.
- Harb Ph (K), Augem M. Synthèse céphalométrique tridimensionnelle (aux trois dimensions de l’espace est associée la quatrième : le temps). SOSortho 108 :5-12, 2002.
- Harb Ph (K). L’orthopédie dento-façiale posturale associée ou non aux dysfonctions articulaires. Inf dent 2003; 39:2949-2960.
- Joerger R. La relation Centrée, un concept métaclinique. Stratégie Proth 2005;5(5):369-376. Cat1.
- Joerger R. Le Gall M.G., Baumann B. Mastication et Déglutition : Tracés axiographiques : Essai Clinique. Cah Prothèse 2012;158:45-54. Cat1.
- Kamina K. Anatomie clinique tête, cou, dos. Tome 2. Troisième édition. Maloine 2006.
- Kamina K. Précis d’anatomie clinique – Tome 2 (MI) édition Maloine 2002.
- Le Gall M, Lauret JF, Joerger R. la fonction occlusale implications cliniques. Editions CDP 2011.
- Le Gall M.G. Physiologic balancing of occlusion. Part one : How can swallowing occlusion be adjusted ? Rev. Odont. Stomat. Sept 2013 ; 42 :198-210.
- Le Gall M.G. Physiologic balancing of occlusion. Part tow : How to adjust posterior occlusal faces ? Rev. Odont. Stomat. Nov 2013 ; 42 :243-257.
- Le Gall M.G. Joerger R., Bonnet B. où et comment situer l’occlsuion ? Relation Centrée ou position de déglutition guidée par la langue ? Cah prothèse 2010 ; 150 : 33-46.
- Le Guern, JY. Etude expérimentale de la répétitivité des contacts occlsuaux sur le chemin de fermeture lors de l’élévation mandibulaire. Intérêt clinique. Thèse Sc. Odontol. 3° Cycle, Nantes, 1987.
- Loreille J.P. Croissance crânio-faciale, Stomatologie-Odontologie II. EMC, 23-455-C-10,1996, 10p.
- Mac Collum B.B. Fundamentals involved in prescribing restorative dental remedies . Dent Items 1939 ;61 :522-35, 641-48, 724-36, 852-63, 942-50.
- Marseillier E. les dents humaines morphologie. Nouveau tirage Edition Gaultier-villars 1958.
- Mongini F. Anatomic and clinical evaluation of the relation-ship between the temporo-mandibular joint and occlusion. prosth.dent 38, 539-551 1977.
- Orthlieb JD. La courbe de Spee : un impératif physiologique et prothétique. Cah Prothèse 1983;44:89-116.
- Orthlieb JD. Gnathologie fonctionnelle vol 1 et 2: Occlusion et restauration prothétique 2009.
- Picq P. La canine humaine: évolution et signification adaptative. Revue Orthop Dento-Faciale 2010 ; 44:9-15
- Romerowski J, Bresson G. Du choix des relations mandibulo-maxillaires en prothèse. Cah Prothèse 1987;59:33-48.
- Salagnac J.M. Développement du rachis cervical et développement facial. Rev Orthop Dento Faciale. 41. 2007. 393-415.
- Slavicek R. Les principes de l’occlusion. Rev Orthop Dento fac 1983; 17:449-90.